Retake
C8) Dyspnea, weight loss, and hemoptysis in a lifelong smoker
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with cough and weight loss.
- Review the DDx considerations in cough and weight loss.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with cough and weight loss.
History
A 65-year-old male with an 80 pack-year smoking history presents to the ED due to new onset back pain. With further history, he endorses chronic cough and new onset productive bloody sputum over the past two months. He also endorses 30lbs of unintentional weight loss, night sweats, decreased appetite, and progressive shortness of breath over the last year. The patient has not seen a physician in more than 20 years.
Physical Exam
BP: 125/80 HR 65, RR 18, Temp, O2 saturation 92%. General: Patient appears cachectic. Pulmonary: Wheezing in right upper lung field. Neuro: Reduced sensation to pinprick in left T3 dermatome. Tenderness to palpation of upper thoracic spine.
Labs
Calcium: 12.3 (8.5 to 10.2mg/dL)
Provisional Diagnosis
Select the Dx you believe is most appropriate
While all these conditions may present with hemoptysis, lung cancer is the most likely considering the chronic onset of constitutional symptoms with significant smoking history. The elevated calcium may be secondary to humoral hypercalcemia of malignancy (HHM). The back pain may be secondary to metastatic deposits.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
While this patient’s condition is not immediately life-threatening, expedited workup is necessary to ensure prompt treatment initiation.
First Imaging Study
What is the first imaging study you will order?
Chest X-ray is the most appropriate initial diagnostic modality and limits radiation burden.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
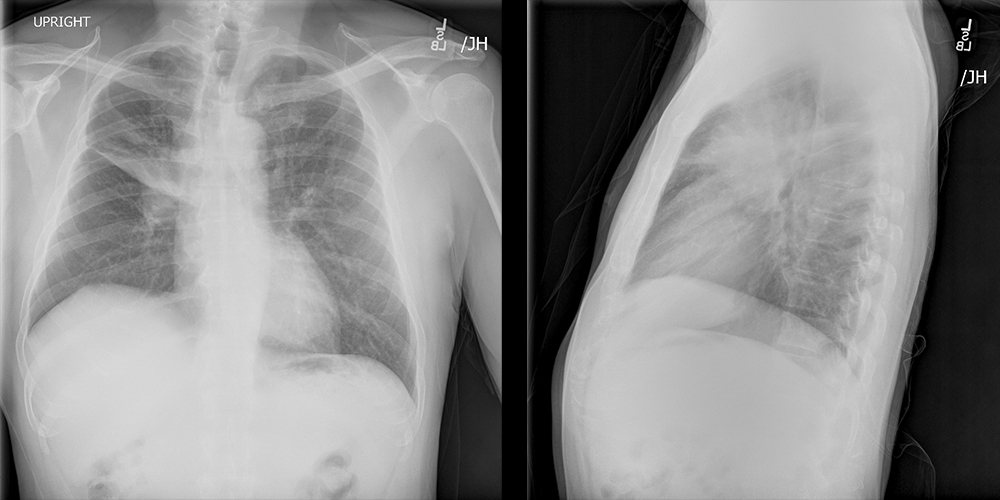
PA and lateral chest X-ray
What best describes the findings on the chest x-ray?
There is a large mass lesion near the hilum of the right lung. Its large size is highly concerning for malignancy. There is also atelectasis of the anterior portion of the right upper lobe. These findings represent atelectasis and not airspace opacifications considering the superior displacement of the minor fissure, absence of air bronchograms, and absence of fluffy infiltrates with indistinct borders.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A chest CT can confirm the presence of a parenchymal mass lesion causing partial lobar atelectasis.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
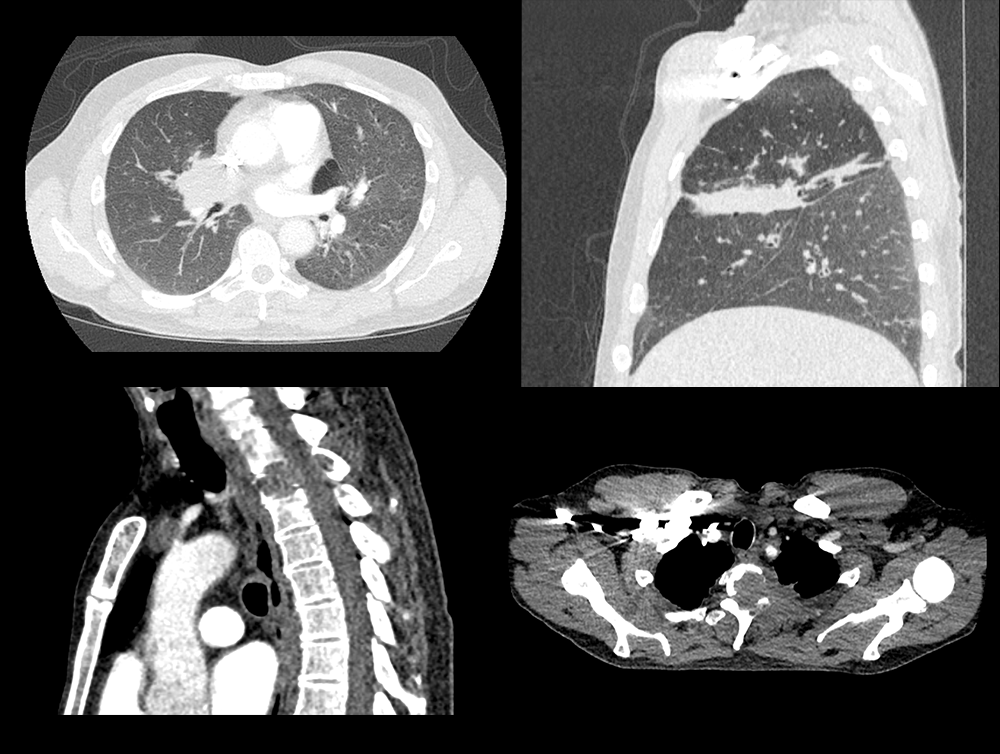
Chest CT
What best describes the findings on the Chest CT?
The CT demonstrates a mass lesion in the near the right hilum resulting in right upper lobe volume loss secondary to obstruction of the right upper lobar bronchus. There is also a destructive lesion at T2 and T3.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
The patient will require a metastatic workup with PET scan. The images are not included here for our purposes. They will also require an MRI to assess for spinal canal involvement of the suspected metastatic lesion.
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
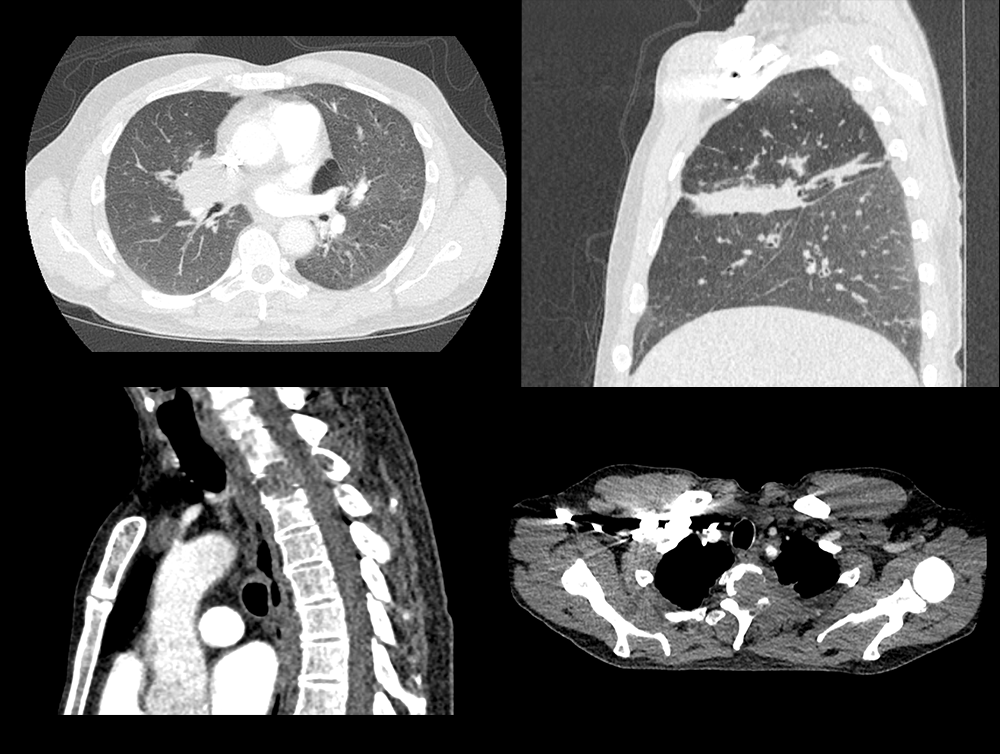
Chest CT
What best describes the findings on the Chest CT?
The CT demonstrates a mass lesion in the near the right hilum resulting in right upper lobe volume loss secondary to obstruction of the right upper lobar bronchus. There is also a destructive lesion at T2 and T3.
What is your Diagnosis now that you have seen the imaging results?
The patient likely has post-obstructive atelectasis and spinal metastases secondary to an endobronchial carcinoma. The patient will require further workup.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This is urgent given need for metastatic workup and the metastatic disease to the thoracic spine with encroachment upon the spinal canal and neurological symptoms.
Assessment and Plan
Please provide your assessment and plan for this patient
65-year-old male with extensive smoking history presenting with back pain, hemoptysis, and constitutional symptoms. Imaging was concerning for endobronchial cancer with partial right upper lobar collapse and T2/T3 metastases with possible spinal cord compression. This is likely a squamous cell carcinoma considering the central location and suspected HHM. The patient will require an urgent MRI of the T spine and a pulmonology consultation for possible endoscopic biopsy of the mass.
Lessons Learned: Squamous cell carcinoma of the lung often presents centrally (near the hilum) and therefore can lead to post-obstructive lobar atelectasis. Squamous cell carcinoma can lead to HHM secondary to over-secretion of parathyroid hormone-related peptide (PTHrP).
Socioeconomic Factors: This case demonstrates the importance of regular screening. The USPSTF recommends annual screening for lung cancer in adults aged 50-80 who have a 20 pack-year smoking history and currently smoke or quit smoking within the last 15 years.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}
{kind=link}